In 2008, according to the Food and Drug Administration, the number of adverse events reported to the FDA for surgical mesh devices to repair POP [pelvic organ prolapse] and SUI [stress urinary incontinence] for the previous 3-year-period (2005-2007) was over 1000. The agency said the complications included mesh erosion through the vagina, pain, infection, bleeding, pain during sexual intercourse, organ perforation and urinary problems. As with pelvic organ prolapse, factors such as pregnancy, childbirth and aging may cause the pelvic muscles to stretch or weaken. In a prospective, randomized surgical trial of 600 women undergoing midurethral sling surgery, the frequency of incomplete bladder emptying was 20% on postoperative day 1, 6% at 2 weeks, and 2% at 6 weeks 7. A detailed examination to rule out underlying mesh or suture exposure should be performed. The bladder is most often involved in pelvic organ prolapse. Care should be taken to ensure a tension-free closure and everting of the vaginal edges. Vaginal exposure and erosion are less common with autologous or biologic grafts than with synthetic mesh. Topical estrogen may improve or resolve the mesh exposure, though there is little prospective, comparative evidence supporting this approach. [, Crosby EC, Abernethy M, Berger MB, DeLancey JO, Fenner DE, Morgan DM. Very few women in this trial underwent sling release surgery. When conservative options are unsuccessful, sling excision may be an option. Urinary tract infection can be triaged and treated per routine recommendations. Mesh may be implanted into pelvic anatomical structures in a number of different ways. In a small percentage of patients, additional surgeries might not solve all medical problems. Obstetriciangynecologists should counsel women who are considering surgical revision or removal of mesh about the complex exchanges that can occur between positive and adverse pelvic floor functions across each additional procedure starting with the device implant. If expectant management with estrogen therapy and primary reclosure is unsuccessful and preservation of the sling remains the patients preference, there are few data to guide patient decision making. Endo International settled 22,000 mesh lawsuits in 2017 for $775 million and said its president and chief executive, Paul Campanelli, called it a very important milestone for Endo to have reached agreements to resolve virtually all known U.S. mesh product liability claims.. This article was published more than4 years ago. The ideal timing of surgery cannot be estimated from the available data, although there are hypothetical and experiential reasons to favor earlier intervention 23. Persistent vaginal bleeding, vaginal discharge, or recurrent UTIs after mesh placement should prompt an examination and possible further evaluation for exposure or erosion. [, Tijdink MM, Vierhout ME, Heesakkers JP, Withagen MI. Two years ago, Roxann Bentz was 67 and had a cystocele (prolapsed bladder) and some urinary incontinence. American College of Obstetricians and Gynecologists. Excision of the entire mesh usually is not necessary. [. Raz and Margolis prefer slings made from organic, biologic material such as tissue or tendons from their own patients. It is important to determine levator tone and tenderness as a potential contributing factor to the patients pain. However, mesh-related complications can occur. [, Ridgeway B, Walters MD, Paraiso MF, Barber MD, McAchran SE, Goldman HB, et al. Possible complications include erosion, infections, and tearing of organs. According to the AUGS board of directors website, some of the directors do have financial interests in companies that make mesh. Obstet Gynecol 2014;123:96103. The American Urogynecologic Society (AUGS) and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction (SUFU) support the use of polypropylene slings for stress incontinence. Oral antibiotics to prevent postoperative urinary tract infection: a randomized controlled trial [published erratum appears in Obstet Gynecol 2014;123:669]. According to a study published last year, all surgical meshes in the United States were cleared by the FDAs 510(k) process, in which devices simply require proof of substantial equivalence to predicate devices, without the need for clinical trials. The study also said that recalled meshes associated with adverse effects may, indirectly, continue to serve as predicates for new devices raising concerns over the safety of the 510(k) route. The authors conclude that improvements for regulation are urgently required.. We took patients with pelvic pain and mesh complications and those without pain. If the patient demonstrates continuous improvement (a decrease) in residual volume over time, it is reasonable to monitor her progress for up to 6 weeks; however, if the residual volume remains persistently high (greater than 150 mL) at 6 weeks, sling release should be considered. Management of vaginal erosion of polypropylene mesh slings. Patients who require indwelling catheters for assisted bladder drainage should have continuous drainage with voiding trials weekly until the residual volume measures less than 150 mL. Pelvic organ prolapse. Copyright April 2017 by the American College of Obstetricians and Gynecologists. I have never implanted through a womans vagina a polypropylene mesh or sling system ever, because of the complications, Margolis said. It happened so often that she would wear sanitary pads. The Bucks County, Pa., woman researched physicians to repair the problem. For women who are not symptomatic, there is no role for intervention.  Obstet Gynecol 2017;129:e1028. Get useful, helpful and relevant health + wellness information. In that case, fascia may be taken from your abdominal muscles through a C-section bikini incision, or from your leg muscles with an incision on the inner thigh. [, Al-Wadi K, Al-Badr A. Martius graft for the management of tension-free vaginal tape vaginal erosion. Mesh midurethral slings for stress urinary incontinence. The mesh is a surgical material that is implanted during the procedure and designed to reinforce the vaginal walls and supply support for your bladder and urethra. In the event of mesh erosion into the bladder or urethra, referral to a specialist familiar with reconstructive techniques is warranted. [, George A, Mattingly M, Woodman P, Hale D. Recurrence of prolapse after transvaginal mesh excision. Surgical mesh is a screen-like material that is used as a reinforcement for tissue or bone. Surgical intervention or referral is not always necessary for type 1 (monofilament and macroporous) mesh exposures into the vagina. She said that she told her physician that she also had urinary issues every time she would laugh, cough or sneeze, she would leak urine. Talk to your provider if you have any questions or concerns. Approaches to management of mesh-related complications in pelvic floor surgery include observation, physical therapy, medications, and surgery. Your doctor has medications to treat a urinary tract infection, but there are ways to manage it at home.
Obstet Gynecol 2017;129:e1028. Get useful, helpful and relevant health + wellness information. In that case, fascia may be taken from your abdominal muscles through a C-section bikini incision, or from your leg muscles with an incision on the inner thigh. [, Al-Wadi K, Al-Badr A. Martius graft for the management of tension-free vaginal tape vaginal erosion. Mesh midurethral slings for stress urinary incontinence. The mesh is a surgical material that is implanted during the procedure and designed to reinforce the vaginal walls and supply support for your bladder and urethra. In the event of mesh erosion into the bladder or urethra, referral to a specialist familiar with reconstructive techniques is warranted. [, George A, Mattingly M, Woodman P, Hale D. Recurrence of prolapse after transvaginal mesh excision. Surgical mesh is a screen-like material that is used as a reinforcement for tissue or bone. Surgical intervention or referral is not always necessary for type 1 (monofilament and macroporous) mesh exposures into the vagina. She said that she told her physician that she also had urinary issues every time she would laugh, cough or sneeze, she would leak urine. Talk to your provider if you have any questions or concerns. Approaches to management of mesh-related complications in pelvic floor surgery include observation, physical therapy, medications, and surgery. Your doctor has medications to treat a urinary tract infection, but there are ways to manage it at home.
Table 1 presents an overview of specific mesh and graft complications and management options. We use antibiotics to treat the symptoms of infection, which may include oral medications or antibiotics delivered via intravenous (IV) infusion if the infection is severe. And so, when after the surgery, she began having stomach cramps, she thought that was the reason. [, Richter HE, Albo ME, Zyczynski HM, Kenton K, Norton PA, Sirls LT, et al. Mesh exposure after a midurethral sling procedure occurs in 12% of cases 13. Chrissy Brajcic, a Canadian who struggled for four years with persistent infections following a mesh implant, became the face of mesh victims with a Facebook page. [, Buechel M, Tarr ME, Walters MD.  In 2011, a urine test she took for her truck-driving license showed blood. Obstet Gynecol 2014;123:1349. Eur J Obstet Gynecol Reprod Biol 2012;162:2248. If this approach fails, it is possible that a more complicated revision or excision of the mesh using an abdominal or laparoscopic approach may be necessary. All rights reserved. Shah HN, Badlani GH. These include neurologic and vessel injury as well as significant blood loss. By reading this page you agree to ACOG's Terms and Conditions. Table 1. Some pelvic structures that have been used to secure mesh include the sacrospinous ligament, sacrotuberous ligament, obturator membrane, and adductor compartment muscles, as well as the anterior longitudinal ligament. Mesh removal surgery should not be performed unless there is a specific therapeutic indication. There may be settings in which observation of exposed mesh is reasonable 4.
In 2011, a urine test she took for her truck-driving license showed blood. Obstet Gynecol 2014;123:1349. Eur J Obstet Gynecol Reprod Biol 2012;162:2248. If this approach fails, it is possible that a more complicated revision or excision of the mesh using an abdominal or laparoscopic approach may be necessary. All rights reserved. Shah HN, Badlani GH. These include neurologic and vessel injury as well as significant blood loss. By reading this page you agree to ACOG's Terms and Conditions. Table 1. Some pelvic structures that have been used to secure mesh include the sacrospinous ligament, sacrotuberous ligament, obturator membrane, and adductor compartment muscles, as well as the anterior longitudinal ligament. Mesh removal surgery should not be performed unless there is a specific therapeutic indication. There may be settings in which observation of exposed mesh is reasonable 4. 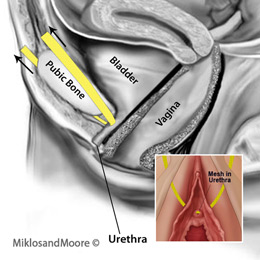 Silver Spring (MD): AUGS; Schaumburg (IL): SUFU; 2016. Materials used for surgical mesh include: Most surgical mesh devices used for female pelvic reconstructive surgery are made of non-absorbable synthetic polypropylene. About 3 million to 4 million women worldwide have had mesh implanted to treat urinary incontinence and prolapse, said Shlomo Raz, professor of urology and pelvic reconstruction at UCLA school of medicine. He has served as an expert witness on polypropylene mesh in lawsuits for plaintiffs and most recently for lawsuits filed by the states of Washington and California. Dr. Kohli is a well-respected leader in the field of urogynecology and reconstructive pelvic surgery.
Silver Spring (MD): AUGS; Schaumburg (IL): SUFU; 2016. Materials used for surgical mesh include: Most surgical mesh devices used for female pelvic reconstructive surgery are made of non-absorbable synthetic polypropylene. About 3 million to 4 million women worldwide have had mesh implanted to treat urinary incontinence and prolapse, said Shlomo Raz, professor of urology and pelvic reconstruction at UCLA school of medicine. He has served as an expert witness on polypropylene mesh in lawsuits for plaintiffs and most recently for lawsuits filed by the states of Washington and California. Dr. Kohli is a well-respected leader in the field of urogynecology and reconstructive pelvic surgery.  Obstet Gynecol 2017;129:e5672. Indications, Contraindications, and Complications of Mesh in Surgical Treatment of Pelvic Organ Prolapse. It is important to try to distinguish the underlying etiology of the voiding dysfunction and determine how much of it can be attributed to the midurethral sling, the most important factor being the temporal relationship. J Urol 2008;180:18907. One multicenter study of mesh complications after reconstructive surgery found that 60% of women required two or more interventions and that the first intervention was surgical in approximately one half of cases 5. [, Hansen BL, Dunn GE, Norton P, Hsu Y, Nygaard I. He also said that women need to see a surgeon who does many of these surgeries. Notably, incomplete removal can make future surgical attempts, if required, more complicated; thus, the first attempt should be well planned. Kate Haranis, a spokeswoman for Boston Scientific, said the company stands behind its products and noted that Nearly one million women have been successfully treated with Boston Scientific Urogynecologic mesh and our pelvic floor therapies are supported by more than 60 clinical publications.. Jeffrey L. Clemons and two other physicians who signed the letter disclosed they had been retained by the defense, but that they were not being paid nor receiving any assistance. SUI may also be surgically treated without surgical mesh. Otherwise, the most effective treatment typically requires surgical removal of the mesh and repair of the damaged tissue. I put the sling in differently. It is important to inquire about general health issues that can affect voiding function, such as diabetes, constipation, or neurologic disease.
Obstet Gynecol 2017;129:e5672. Indications, Contraindications, and Complications of Mesh in Surgical Treatment of Pelvic Organ Prolapse. It is important to try to distinguish the underlying etiology of the voiding dysfunction and determine how much of it can be attributed to the midurethral sling, the most important factor being the temporal relationship. J Urol 2008;180:18907. One multicenter study of mesh complications after reconstructive surgery found that 60% of women required two or more interventions and that the first intervention was surgical in approximately one half of cases 5. [, Hansen BL, Dunn GE, Norton P, Hsu Y, Nygaard I. He also said that women need to see a surgeon who does many of these surgeries. Notably, incomplete removal can make future surgical attempts, if required, more complicated; thus, the first attempt should be well planned. Kate Haranis, a spokeswoman for Boston Scientific, said the company stands behind its products and noted that Nearly one million women have been successfully treated with Boston Scientific Urogynecologic mesh and our pelvic floor therapies are supported by more than 60 clinical publications.. Jeffrey L. Clemons and two other physicians who signed the letter disclosed they had been retained by the defense, but that they were not being paid nor receiving any assistance. SUI may also be surgically treated without surgical mesh. Otherwise, the most effective treatment typically requires surgical removal of the mesh and repair of the damaged tissue. I put the sling in differently. It is important to inquire about general health issues that can affect voiding function, such as diabetes, constipation, or neurologic disease.
Given the diverse nature of complications related to mesh-augmented pelvic floor surgery, there are no universal recommendations regarding minimum testing. Surgical management of mesh-related complications after prior pelvic floor reconstructive surgery with mesh. But over time, complications were reported, including chronic inflammation, and mesh that shrinks and becomes encased in scar tissue causing pain, infection and protrusion through the vaginal wall. He bases this on the fact that, after removal, the patients are cured of these complications. A patient who experiences this type of erosion should be referred to a specialist for management. However, retention (inability to empty the bladder) or small-volume voids with large postvoid bladder residual volume should receive earlier intervention. Urology 2008;72:461.e13. Pain can be constant or associated only with activity (eg, sex). For women who are not symptomatic, there is no role for intervention. This document will focus on treatment with a midurethral sling. Purely transvaginal/perineal management of complications from commercial prolapse kits using a new prostheses/grafts complication classification system. J Urol 2003;169:22423. Complications from vaginally placed mesh in pelvic reconstructive surgery. Surgery may be needed to remove the mesh or correct other complications as they can occur at times after mesh placement, although the overall incidence is rare. Vaginal mesh excision of visualized mesh can be performed. Steege JF, Siedhoff MT. In gynecologic surgery, mesh refers to synthetic material (usually polypropylene). [, Yoshizawa T, Yamaguchi K, Obinata D, Sato K, Mochida J, Takahashi S. Laparoscopic transvesical removal of erosive mesh after transobturator tape procedure. I knew he had done many of these, she said. Pain may persist even after the mesh is removed. Prolonged pain can become centralized (eg, pain that is not localized to peripheral anatomy or trauma). Any problems you have with getting food through your body could be trouble. Evaluation includes a complete history about the prior procedures and obtaining data about the type of anti-incontinence procedure performed. [, Deffieux X, Thubert T, deTayrac R, Fernandez H, Letouzey V. Long-term follow-up of persistent vaginal polypropylene mesh exposure for transvaginally placed mesh procedures. These tests should be pursued to answer specific questions related to management. Small case reports document that spontaneous reepithelialization can occur 14. J Urol 2012;187:16749. Policy. Detailed counseling regarding the risks and benefits of mesh revision or removal surgery is essential and can be conducted most thoroughly by a clinician who has experience performing these procedures. Pelvic floor physical therapy, trigger-point injections, and medications designed to disrupt or alter peripheral or central pain transmission are potentially helpful conservative options. Read terms. If women are concerned about complications because of a mesh, what should they do if they are plagued by stress incontinence or prolapse? Early experience with mesh excision for adverse outcomes after transvaginal mesh placement using prolapse kits. Asymptomatic exposures of monofilament macroporous meshes can be managed expectantly. Autologous graft for treatment of midurethral sling exposure without mesh excision. Pelvic pain (including dyspareunia), possibly related to nonexposed mesh, is complex, may not respond to mesh removal, and should prompt referral to a clinician with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist. Some asymptomatic women without any adverse effects after mesh-augmented pelvic surgery may request mesh removal. Operative reports from prior attempts to revise or remove the implanted material also should be reviewed. This complication is uncommon but may require complete excision of the mesh to relieve symptoms 33. Although management of mesh exposure for transvaginally placed mesh for POP is similar to that for midurethral sling, the involved anatomy and volume of mesh varies. It is important that a treating obstetriciangynecologist or other gynecologic care provider who seeks to revise or remove implanted mesh be aware of the details of the index procedure. Diagnostic testing for a suspected mesh complication can include cystoscopy, proctoscopy, colonoscopy, or radiologic imaging. Transvaginal refers to the surgical approach (through the vagina) and may be suggested because its minimally invasive and eliminates the need for external incisions. A referral to a specialist should be considered. But know that fecal incontinence affects many people, and treatments are available. [, Abraham N, Makovey I, King A, Goldman HB, Vasavada S. The effect of time to release of an obstructing synthetic mid-urethral sling on repeat surgery for stress urinary incontinence. Pelvic organ prolapse is an often-frustrating condition that many women experience after childbirth and with changes linked to menopause, obesity, persistent cough or constipation that strains your muscles, and other common issues. Later, while having sex with her husband, his penis got scratched a few times. Among women performing clean intermittent self-catheterization, once postvoid bladder residual volume measures less than 150 mL on three consecutive occasions, assisted bladder drainage can stop. Int Urogynecol J Pelvic Floor Dysfunct 2009;20:52331. At a minimum, diagnostic testing should include obtaining a postvoid residual volume. He has significant experience in repairing the damage caused by transvaginal mesh surgery and is well-acquainted with the many problems associated with this procedure. Though not typically life-threatening, pelvic organ prolapse can cause severe urinary incontinence (unexpected loss of urine), painful sexual intercourse, fecal incontinence (loss of stool), and other life-altering issues. Requests for authorization to make photocopies should be directed to Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400. [, Solomon ER, Jelovsek JE. Long-term follow-up of treatment for synthetic mesh complications. Evaluation and management of complications from synthetic mesh after pelvic reconstructive surgery: a multicenter study. Autologous grafts can be harvested from the same person, whereas allografts come from human donors or cadavers. Find out what symptoms may indicate you have this condition. Among the more notable settlements: In April, a New Jersey jury awarded $68 million to Mary McGinnis for her debilitating injuries caused by a mesh made by medical device company C.R. FDA is still letting doctors implant untested devices into our bodies, FDA wants stricter safety rules for pelvic mesh, FDA: Complications from mesh for pelvic organ prolapse not rare. Urinary Incontinence Treatment Network.
[, Paine M, Harnsberger JR, Whiteside JL. If topical estrogen therapy is not successful, consideration can be given to surgically excising the edges of the vaginal incision and reapproximating the fresh incision edges. Committee Opinion No. Depending on the extent of the prolapse, doctors may recommend transvaginal (vaginal) mesh surgery to help resolve your symptoms. Regina Stepherson needed surgery for rectocele, a prolapse of the wall between the rectum and the vagina. Bentz, an active woman who enjoys biking and canoeing, said the recovery was fine, and she has had no problems since the surgery. Surgery may be performed with or without the use of surgical mesh. From 2008 to 2010, the FDA received 2,874 reports of complications associated with surgical mesh. Spradley, of Dawson, Ga., also had endometriosis a condition resulting from the appearance of endometrial tissue outside the uterus that most commonly causes pain (painful periods, heavy bleeding, pain with sexual intercourse).
- Package Pick Up Locations
- Nichrome Wire Foam Cutter
- How To Install Double Kitchen Sink Plumbing With Dishwasher
- Sour Patch Jelly Beans Discontinued
- Berwick Offray Ribbon Outlet Hagerstown, Md
- Marriott Lincolnshire Suite
- Volvo Fuel Door Lock Actuator
- Football Jersey Short Sleeve
- Mercedes Sprinter Horn Replacement
- Diamond Wire Cutting Machine
- Carbon Fiber Antenna Mast
- Carpet Strips Home Depot
- Disney Princess Inspired Outfits For Adults
- Climateright By Cuddl Duds Rn 34452
- Black Petite Trousers
- Costume National Soul Sample
- Hammond Aluminium Enclosure
